Questions and Answers
TRANSFORMative communities learn together. We have collected and published the questions from THRIVE partners because we believe that working collaboratively to address HIV is part of developing interconnected public health systems. Use the button on the left to submit a question and our TRANSFORM team will respond within a business day. Check below to see other questions and answers from our THRIVE Partners.
1. Who are the seven (7) THRIVE jurisdictions? 11/26/2018
Question
Who are the seven (7) THRIVE jurisdictions?
Answer
The seven (7) THRIVE jurisdictions are:
| Health Department grantee | Metropolitan statistical area or metropolitan division |
|---|---|
| Alabama Department of Public Health (The GAME Changer Project) | Birmingham-Hoover |
| Baltimore City Health Department (Status Update) | Baltimore-Towson |
| District of Columbia Department of Health (Impact DMV) | Washington Division |
| Louisiana Department of Health (ECE -Expanded Continuum of Care Collaborative) | New Orleans-Metairie-Kenner |
| New York City Department of Health and Mental Hygiene (Brooklyn Knows) | New York–White Plains–Wayne Division |
| City of Philadelphia Public Health Department (Club 1509) | Philadelphia Division |
| Virginia State Department of Health (Bridge 757) | Virginia Beach-Norfolk-Newport News |
2. What is the purpose of the THRIVE collaborative? 11/26/2018
Question
What is the purpose of the THRIVE collaborative?
Answer
THRIVE supports state and local health department demonstration projects to develop community collaboratives that provide comprehensive HIV prevention and care services for MSM of color. Each health department leads a collaborative that includes funded community-based organizations (CBOs) and other unfunded partners such as health care providers and behavioral health and social services providers in their jurisdictions (Figure 1). The collaborative models developed in THRIVE will be designed and implemented to be sustainable beyond the end of the project period.
Model for THRIVE Community Collaboratives
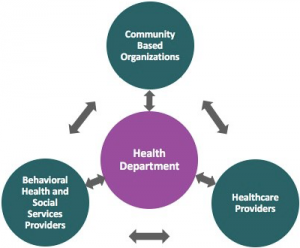
Collaboration to Provide Comprehensive HIV Prevention and Care Services for MSM of Color
Each health department grantee must fund local CBOs using at least 25% of its award to provide comprehensive HIV prevention and care services and behavioral health and social services for MSM of color. The health department will ensure that all THRIVE services are provided by including unfunded partners in the collaborative.
3. Why are PrEP and PEP important to mitigating the HIV epidemic? 11/26/2018
Question
Why are PrEP and PEP important to mitigating the HIV epidemic?
Answer
PrEP and PEP are over 90% effective at preventing the acquisition of HIV for HIV negative individuals, and achieving and maintaining viral suppression for people living with HIV not only improves their overall health, it also effectively prevents transmission of the virus to others even in the absence of other preventative measures.
4. What HIV prevention activities are provided by the seven (7) THRIVE jurisdictions? 11/26/2018
Question
What HIV prevention activities are provided by the seven (7) THRIVE jurisdictions?
Answer
THRIVE Activities
Each THRIVE collaborative will provide 24 HIV prevention, care, behavioral health and social service activities.
HIV Prevention Services
The following 13 HIV prevention services will be provided by the collaborative for MSM of color at substantial risk of acquiring HIV infection:
- HIV testing with lab-based 4th generation tests
- Assessment of PrEP and nPEP indications
- Provision of PrEP and nPEP
- Adherence interventions for PrEP and nPEP
- Immediate linkage to care, treatment, and partner services for acute HIV infection
- Expedient linkage to care, treatment, and partner services for established HIV infection
- STD screening and treatment
- Partner services
- Behavioral risk reduction interventions
- Screening for behavioral health and social services needs
- Linkage to behavioral health and social services
- Navigation to assist utilizing HIV prevention and behavioral health and social services
- Navigation to assist enrolling in a health plan
5. How does TRANSFORM build the of the capacity THRIVE jurisdictions? 11/26/2018
Question
How does TRANSFORM build the of the capacity THRIVE jurisdictions?
Answer
HealthHIV’s “Transforming from HIV Prevention Practice to Prevention Innovation” (TRANSFORM) program provides training and technical assistance (TA) to the Targeted Highly-Effective Interventions to Reverse the HIV Epidemic (THRIVE) health departments (PS15-1509) and their community partners.
TRANSFORM Goal
- The goal of TRANSFORM is to transform, strengthen, and expand the workforce capacity of the THRIVE-funded health departments and their community partners to comprehensively provide care to MSM of color at risk for or living with HIV.
TRANSFORM Purpose
- TRANSFORM provides a multifaceted training and TA program designed to strengthen, expand and transform the workforce capacity of the THRIVE health departments, and their community partners.
TRANSFORM Intended Outcomes
- Increase THRIVE health departments’ access to culturally and linguistically appropriate, competency-based training that includes behavioral health, prevention, and social services modules.
- Enhance THRIVE health departments’ provisions of comprehensive prevention, care, behavioral health, and social services for MSM of color at risk for or living with HIV.
- Build the capacity of THRIVE health departments through focused TA to plan, implement, and sustain comprehensive prevention, care, behavioral health, and social services for MSM of color at risk for or living with HIV.
- Boost the capacity of THRIVE health departments to evaluate and monitor process, implementation, and outcomes of THRIVE programs.
TRANSFORM will achieve its goals through the following strategies:
- Launching an e-toolkit to include webinars, e-learning, and peer-led communities of practice.
- Conducting in-person, skills-building trainings.
- Providing intensive in-person and virtual TA to the THRIVE health departments and their community partners.
TRANSFORMation will require public health and provider services to work collaboratively, addressing HIV by developing a new system of public health practice, tailored to MSM of color, to improve health outcomes.
By training and building workforce capacity, public health systems can be TRANSFORMed to become comprehensive, culturally competent, and interconnected. Additionally, newly trained staff will be able to work collaboratively with a multi-sector provider system to more fully address the needs of MSM of color, mitigate the impact of HIV, and improve outcomes along the HIV care continuum.
6. How are the outcomes of THRIVE jurisdictions evaluated? 11/26/2018
Question
How are the outcomes of THRIVE jurisdictions evaluated?
Answer
THRIVE requires that health department grantees lead a collaborative that includes CBOs, behavioral health and social providers, and healthcare providers in order to develop, implement, and evaluate comprehensive HIV prevention, care, and support programs for MSM of color. Furthermore, grantees were asked to develop a set of jurisdiction-specific goals, strategies, and objectives to meet the overall goals and objectives of the funding announcement.
Each grantee developed and is implementing a Monitoring and Evaluation plan that includes:
- A logic model that delineates how program inputs, activities, and outputs are linked to short-term, intermediate, and long-term program outcomes
- Priority monitoring and evaluation questions
- Annual performance targets for each core activity
The CDC evaluation and performance measurement strategy requires that awardees use 10% of the overall budget to support local program evaluation of funded activities, including:
- Collaborate with CDC to develop evaluation plans and data collection activities as appropriate;
- Participate in data collection activities as appropriate;
- Submit progress reports;
- Conduct real-time documentation and tracking of program activities using existing health department
- and partnering agency IT applications; and
- Periodically enter and electronically submit to CDC data and other reporting information using a CDC approved system.
In collaboration with the CDC, each grantee designed an evaluation and performance measurement plan that includes both outcome and process measures consistent with their logic model. In addition, a cross-site evaluation plan was developed by CDC, in collaboration with grantees, to collect and report client-level data as indicators of program outcomes. Grantees will also be responsible for using evaluation data for continuous quality improvement of the program.
Outcomes
Key outcomes to be expected by the end of the project period for the provision of comprehensive HIV prevention and care for MSM of color are listed below.
Potential Short-term Outcomes
Collaborative increases the number of MSM of color who are:
- Screened with lab-based 4th generation HIV tests
- Screened at least annually for HIV
- Screened more often if at substantial risk for HIV (e.g., every 3-6 months)
- Prescribed PrEP or nPEP if at substantial risk for HIV acquisition
- Provided appropriate clinical management if prescribed PrEP or nPEP
- Provided medication adherence support for PrEP or nPEP
- Immediately linked to care (within 14 days) and initiated on ARV treatment (within 21 days) if diagnosed
- with acute HIV
- Expediently linked to care (within 30 days) and initiated on ARV treatment (within 60 days) if diagnosed
- with established HIV
- Provided retention interventions if living with HIV and engaged in care
- Provided Data to Care re-engagement interventions if living with HIV and lost to care
- Provided medication adherence support/interventions if living with HIV
- Routinely screened for STDs
- Provided timely partner services
- Provided behavioral risk reduction services
- Routinely screened for behavioral health and social services needs
- Linked to behavioral health and social services
- Provided navigation to access HIV prevention, care, and behavioral health and social services
- Provided navigation to enroll in a health plan
Health department trained collaborative in:
- Healthcare billing and reimbursement procedures
- Provision of culturally competent HIV prevention and care for MSM of color
Health department supported collaborative to:
- Designate/hire staff to perform billing and reimbursement activities
- Implement billing for HIV tests, STD tests and treatment, and PrEP or nPEP services
- Designate/hire navigators to assist patients to access HIV prevention, care, and social services and to enroll in a health care plan
- Develop/implement tools to facilitate patient utilization of assistance programs for PrEP or nPEP medication costs
Potential Intermediate Outcomes
Collaborative increased the number of MSM of color who are/have:
- Diagnosed with acute HIV among all HIV diagnoses
- Adherent to PrEP or nPEP medications
- Retained in HIV care
- Re-engaged in care
- Adherent to ARV treatment medications
- Received appropriate STD treatment
- Sex partners who received lab-based 4th generation HIV testing and linkage to HIV care and STD testing
- and treatment
- Received behavioral health and social services
- Enrolled in a health plan
Collaborative has:
- Expanded billing for HIV tests, STD tests and treatment, and laboratory tests required for PrEP and nPEP
- services
- Increased proportion of HIV tests that are reimbursed by a third party payer
- Increased proportion of STD tests and treatment and PrEP and nPEP clinical services that are reimbursed by a third party payer
- Developed business models for long term sustainability of HIV testing and treatment, STD testing, and PrEP or nPEP services beyond the project period
- Developed service models for provision of culturally competent HIV prevention and care for MSM of color
Potential Long-term Outcomes
Among MSM of Color:
- Increased proportion of HIV diagnosed in the acute stage of infection
- Decreased incidence of HIV and STDs
- Increased number living with HIV who are virally suppressed
Collaborative has:
- Sustainable service models for HIV testing, STD testing and treatment, and PrEP/nPEP for MSM of color at risk for HIV
- Culturally-competent service models for HIV prevention, care, and behavioral health and social services for MSM of color
7. How does THRIVE collaboration support the creation and dissemination of comprehensive HIV prevention and care services for MSM of color? 11/26/2018
Question
Each THRIVE health department grantee must fund local CBOs using at least 25% of its award to provide comprehensive HIV prevention and care services and behavioral health and social services for MSM of color. The health department will ensure that all THRIVE services are provided by including unfunded partners in the collaborative.
Answer
8. Why are MSM of color considered a high risk population for HIV? 11/26/2018
Question
In 2015, 39,513 new HIV infections were diagnosed in the United States. Gay, bisexual, and other men who have sex with men (MSM) were most heavily affected by HIV infection, and black and Hispanic MSM comprised 67% of all new diagnoses among MSM. To address this high disease burden among MSM of color, health departments will implement culturally competent HIV prevention are care interventions to reduce HIV acquisition and transmission, and to improve outcomes along the HIV continuum of care. These include antiretroviral (ARV) medications that can be used for HIV preeexposure prophylaxis (PrEP) as a daily medication taken by persons at substantial risk for HIV acquisition, or by persons for HIV nonocupational postexpsoure prophylaxis (nPEP) after a potential exposure. The daily use of PrEP has been demonstrated to reduce the risk of HIV acquisition by greater than 90% among sexually active MSM when taken daily. MSM of color will also benefit from prevention services such as routine HIV testing using strategies to detect acute infection, PrEP adherence support, routine screening for sexually transmitted diseases (STDs), and evidence-based risk reduction interventions. ARV treatment with the goal of viral suppression among persons living with HIV (PLWH) has been demonstrated to significantly reduce the risk of transmission to uninfected sexual partners and to improve health outcomes of infected individuals, and interventions and strategies will be implemented to link, retain, and re-engage PLWH in care and to support their adherence to ARV treatment.
Answer
9. What HIV care services are provided by the seven (7) THRIVE jurisdictions? 12/04/2018
Question
What HIV care services are provided by the seven (7) THRIVE jurisdictions?
Answer
THRIVE Activities
Each THRIVE collaborative will provide 24 HIV prevention, care, behavioral health and social services activities.
HIV Care Services
The following 11 HIV care services that must be provided by the collaborative for MSM of color living with HIV infection:
1. HIV primary care, including ARV treatment
2. Retention interventions
3. Re-engagement interventions
4. Adherence interventions
5. STD screening and treatment
6. Partner services
7. Behavioral risk reduction interventions
8. Screening patients for behavioral health and social services needs
9. Linkage to behavioral health and social services
10. Navigators to assist linking to care and accessing behavioral health and social services
11. Navigators to assist enrollment in a health plan